Please wait
Please wait
Zenker diverticulum is a rare but well-known cause of chronic dysphagia with frequent regurgitation of undigested food, chronic cough and risk of aspiration and pneumonia especially in older ages.
It supposed for a sac prolapsing through the hypopharynx and upper esophageal sphincter, which contains food from older meals and producing difficulty or pain in swallowing, regurgitation of undigested food, pressure and difficulty in breathing as well as dysosmia. It occurs more frequently to men, older ages, while it can be undiagnosed for years.
Symptomatology
Diagnosis is usually made by gastroenterologist, during gastroscopy, while an experience endoscopists under direct vision with modern flexible videoendoscopes can visualize the entrance of the Zenker diverticulum.
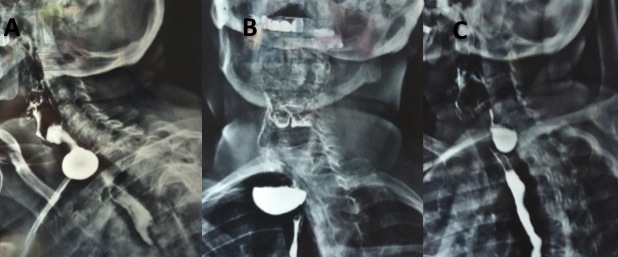
Esophagogram is the examination of choice for diagnosis. During esophagogram the patient swallows contrast medium, which opacifies the hypopharynx and upper esophagus, while it shows the shape and size of the Zenker diverticulum.
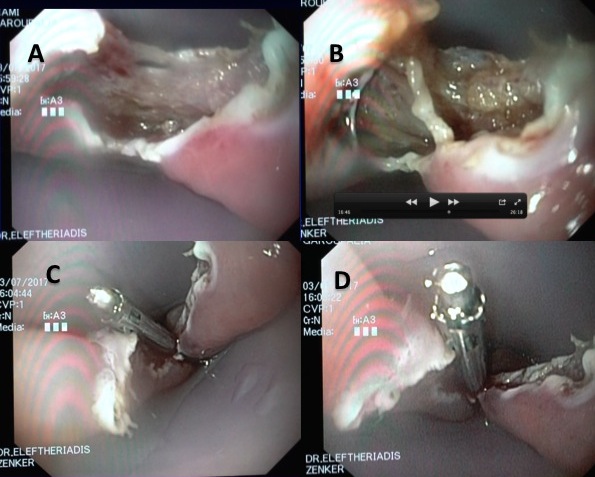
Zenker diverticulum is caused by spasm of cricopharyngeal muscle and obviously radical therapy sould be the myotomy of the responsible muscle, which nowadays is performed within minutes, during gastroscopy with modern flexible video endoscopes, with the most synchronous, minimal invasive, innovative, bloodless, painless, and without scar endoscopic myotomy. Flexible videoendoscopes allows gastroenterologists to approach under direct vision easily the responsible area of hypopharynx and upper esophagus.
With this method, myotomy of the responsible muscle for Zenker diverticulum, is performed endoscopically with special small knives, which pass through the working channel of gastroscope, and so it can be successfully applied tο all cases of Zenker diverticulum, in contrast to older and outdated techniques applied by ENTs using rigid instruments.
Endoscopic myotomy for Zenκer diverticulum (diverticulotomy) is performed during a simple gastroscopy, patients mobilized soon after procedure, starting drinking the next day, and return to all their daily activities directly within a few days.
Major advantages of endoscopic myotomy for Zenker diverticulum are the direct mobilization, short hospitalization (discharge the next day after procedure), immediate feeding with fluids and shoft diet next day after procedure and rapid recovery within few days giving permanent long-term solution even in elderly and debilitating patients.
The interventional gastroenterologist Dr. Nikos Eleftheriadis, successfully applied routinely, the endoscopic myotomy for Zenker diverticulum (diverticulotomy) during gastroscopy, even for large size (>3cm), such as in a 60-years-old female patient, showed below in figures 1-3. This particular patient complained for severe dysphagia for years and chronic cough due to frequent episodes of aspiration due to Zenker diverticulum (images shown in figures 1-3).
Endoscopic myotomy for Zenker diverticulum with gastroscopy, however, is not widespread in Greece due to the scarcity of the disease, obviously the competition from other older and outdated techniques, such as surgical or myotomy with rigid instruments performed by ENT doctors, but also the high training cost, leading many patients to older and outdated techniques with frequent failures and severe complications. As a result many patients with Zenker deprived from the simple and effective method of diverticulotomy with gastroscopy.
The following figures (1-3) are personal cases of Dr. Nikos Eleftheriadis, in which endoscopic Ζenker myotomy (diverticulotomy) was successfully applied during gastroscopy.

NIKOLAOS P. ELEFTHERIADIS
Interventional Gastroenterologist
Specialist in Endoscopic Myotomy (POEM) for Achalasia
Scientific Associate Digestive Disease Center
Showa University Koto-Toyosu Tokyo Japan
Address: Politechniu 3 Triandria, Thessaloniki PC 55337
Tel: (+30) 2311-283002, (+30) and (+30) 6977778832.
Email: nikolaseleftheriadis@gmail.com
Dr. Nikolaos Eleftheriadis performs interventional – therapeutic endoscopies
including POEM & ESD at Metropolitan Hospital in Athens and
at the Kyannous Stavros – Euromedica Clinic in Thessaloniki.